Malnutrition Care Score for IQR
The Malnutrition Care Score quality measure is available for 2025 hospital reporting.
The MQii is designed to help your organization improve
malnutrition care and subsequently achieve better outcomes.
The Malnutrition Care Score quality measure is available for 2025 hospital reporting.
The MQii is designed to help your organization improve
malnutrition care and subsequently achieve better outcomes.
The Malnutrition Quality Improvement Initiative (MQii) aims to advance evidence-based, high-quality malnutrition care for patients who are malnourished or at-risk for malnutrition. The MQii is a project of the Academy of Nutrition and Dietetics, Avalere, and other stakeholders who provided expert input through a collaborative partnership to advance malnutrition care across the nation.
The MQii offers a Toolkit which provides tools and resources to help your organization understand malnutrition care best practices, as well as guidance to help your facility identify quality improvement opportunities and critical gaps. The Toolkit can assist you in generating leadership support for a quality improvement project, building an interdisciplinary Project Team, and implementing the changes needed to advance malnutrition care in your hospital. The MQii also offers a set of de novo malnutrition electronic clinical quality measures (eCQMs) to assess the current quality of care at your institution and monitor changes in the quality of care delivered over time. The Toolkit and eCQMs are intended to mutually support your facility as you implement a quality improvement project and assess the impact on your care.
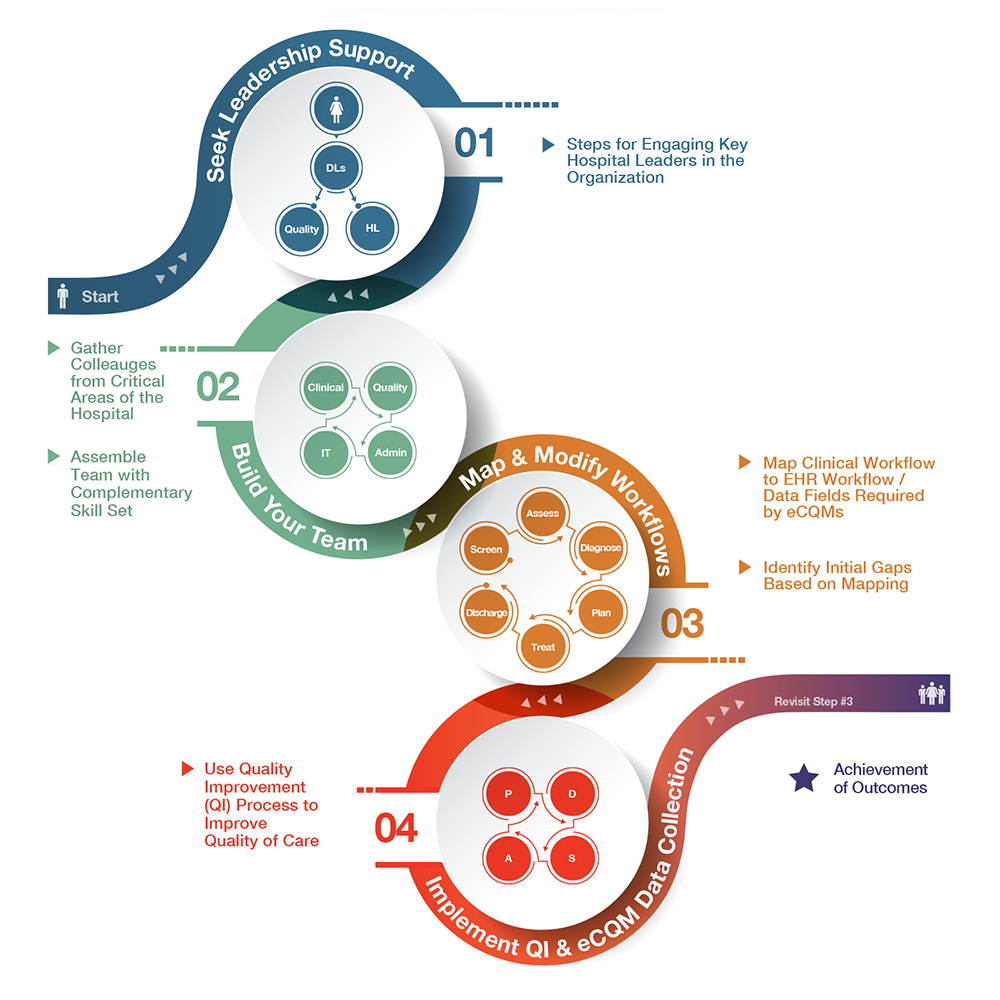
The MQii provides a framework for you to identify malnutrition care gaps at your hospital, introduce a QI project to improve care, and assess progress on the changes implemented. The tools provided through the MQii offer timely, structured, efficient, and evidence-based guidance to inform your QI strategy.
Hospitals across the United States have had success advancing the quality of malnutrition care their patients experience through their participation in the MQii, with the overarching goal of improving patient outcomes and reducing burden to the system.
It is very important to seek leadership support and approval in order to begin an MQii project. The MQii Team is happy to provide you with a “How to Get Started Checklist” that outlines a high-level step-by-step guide to help you undertake a project at your facility. The Value of Quality Malnutrition Care Briefing provides the business case for your leadership and will be a crucial part of gaining their support.
Yes, anyone can undertake a malnutrition QI project—even with little or no experience in quality improvement efforts. Many facilities that have engaged in MQii projects to date have implemented changes with little experience and have done so in the midst of IT upgrades, leadership changes, and staffing shortages. Sites, particularly those dealing with other competing projects or internal challenges, typically have the greatest success starting with a small, manageable project (e.g., within one hospital unit or primarily engaging with one clinician group) and building out from there.
Share the business case and the evidence included in the Value of Quality Malnutrition Care Briefing with your hospital or health system’s leadership to showcase the benefits of participating in the MQii and addressing malnutrition care gaps. Give each of them a copy and tell them you want to start a malnutrition quality improvement project at your hospital. You can also use the “MQii Overview” PowerPoint presentation to help convey the burden of malnutrition on the hospital system and why implementing a malnutrition QI project is an important step to potentially improve patient outcomes such as rates of readmissions, pressure ulcers, and falls, among others. Schedule a meeting with your Quality and Executive teams and discuss these resources with them and make the case for this project.
Electronic clinical quality measures use data from electronic health records (EHRs) and/or health information technology systems to measure and quantify healthcare quality. The Centers for Medicare & Medicaid Services (CMS) use eCQMs in a variety of quality incentive programs and to publicly report data about quality. Measuring and reporting eCQMs helps ensure that care is delivered in a safe, effective, equitable, and timely manner.
The MQii Toolkit is an evidence-based, patient-centered set of resources, tools, and information to help hospitals support malnutrition quality improvement (QI) and implement malnutrition care best practices. The Toolkit provides resources for all members of the care team (e.g., dietitians, nurses, physicians, patients, and caregivers) who engage in care for patients who are malnourished or at risk of malnutrition. It spans all steps in the malnutrition clinical workflow, from screening through assessment, care plan development, diagnosis, monitoring and evaluation, and discharge planning. The Toolkit was built to support malnutrition QI for hospitalized older adults (ages 65 and older), but the majority of tools and resources are relevant and applicable to any adult hospitalized patient and may have implications for post institutional care as well. By supporting malnutrition QI using guidance from this Toolkit, hospitals may be able to:
The MQii is based on the nutrition care process. To start, use the sample flow chart for recommended malnutrition care and the flowchart template, and/or answer the questions in the MQii Nutrition Care Opportunity Assessment to evaluate your current care delivery and determine on which aspect(s) of the workflow your institution will focus its quality improvement efforts. These tools can help your facility determine how your current workflow process compares to the recommended workflow, identify where gaps exist in your current process, and select the best areas in your workflow to target for improvement. The number of aspects of the recommended clinical workflow your organization tackles is up to your Project Team.
The number of components of the recommended clinical workflow your organization tackles is up to your Project Team. Using the resources to support with project prioritization will allow you to identify those target areas where you can direct resources and efforts towards.
You will need to work with your facility’s IT staff to verify that the data elements required to calculate the MQii eCQMs currently exist in your EHR. For sites with Epic, Cerner, or AllScripts installations, most of these EHR versions can collect the necessary patient data to report on the eCQMs, and many organizations are already collecting much of the required data. Therefore, if your site employs a recent version of Cerner, Epic, or AllScripts EHR platforms, it is very likely that your existing system has some capability to collect on the measures’ required data elements.
Should you choose to collect information on one or more of the eCQMs, you will need to involve your IT staff and/or EHR maintenance team to input the specifications into your facility’s EHR platform. In the event that the data elements exist but are not coded to the appropriate specifications, you will need to re- label the applicable data elements to the structured code sets outlined in the measure specifications.
The MQii also provides a data report template to enable you to assess your facility’s ability to collect necessary data elements, and a performance calculator to help you rapidly aggregate and analyze your data to determine your performance.
The MQii resources are intended to be used by all clinicians that play a role in addressing the nutritional needs of hospitalized patients. As such, you are encouraged to identify an interdisciplinary MQii Project Team to facilitate your malnutrition QI project. The Project Team should have a project manager, as well as project champions from dietitian, physician, and nurse clinician groups at a minimum. These clinician leads will assist with the education and training of care team members who will be implementing the changes and will liaise with other clinicians to address any questions.
If you will be collecting data to evaluate your performance, you will also want to include an IT resource on the Team. The IT resource will be expected to pull relevant data elements from the facility’s EHR and ideally be able to manipulate the EHR system to program the specifications of the eCQMs, or make changes to accommodate new data elements (if necessary). Finally, for the greatest likelihood of success, you are strongly recommended to engage a representative from your hospital’s Quality Department and a senior or executive leader with decision-making authority to facilitate necessary internal stakeholder engagement. Ideally, the Project Team members will be familiar with and have experience implementing quality improvement (e.g., using Lean, Six Sigma, Plan-Do-Study-Act models), but this is not a requirement.
The time commitment for your hospital and the Project Team will vary depending on the scope of the project and each individual’s role in the project. It is likely you will need to commit more time as you begin your project to support training and education on your desired change and establish any data collection processes. The time commitment typically decreases following the start of implementation as the project infrastructure is already in place; tasks will become focused on addressing follow-up questions or training needs from clinicians and performing periodic data pulls. The time commitment will also vary depending on how many QI interventions you plan to implement and how many clinicians or units within the hospital you plan to involve.
It is important to note that the time commitment for each Project Team member will vary based on his or her role. For instance, the project manager may spend a few hours per week training staff on best practices in malnutrition care, tracking and monitoring changes in clinical practice, and supporting the Project and care teams. Following implementation, he or she may also spend time analyzing the data, reviewing feedback reports, assessing progress, and advising on what to do next. By contrast, the time commitment for a care team member (e.g., dietitian, nurse, physician) not in a leadership role on the team will be minimal, as they will primarily be spending time receiving initial training and familiarizing themselves with the best practices and how to implement them.
There are no fees associated with participating in the MQii to implement a malnutrition quality improvement, or to access the MQii tools and resources.
A central aspect of quality improvement is to collect data to identify your facility’s baseline performance, assess changes over time, and inform aspects of care that might require further training or education for clinicians. You can use the four MQii eCQMs to collect data regarding rates of malnutrition screening, assessment, care plan development, and diagnosis at your facility and assess changes over time. This may be done through direct extraction of the data from the EHR using the eCQM technical specifications.
The eCQMs were developed with significant multi-stakeholder input, including from advisors in malnutrition care and quality improvement and a Technical Expert Panel. After development, the measures were tested for feasibility, validity, and reliability throughout 2016 in accordance with testing processes recommended by the National Quality Forum (NQF). Feasibility testing took place in three health systems and three different EHR vendors. Subsequently, validity and reliability testing took place within two health systems.
A manuscript was published in a peer-reviewed journal describing the testing approach and results. In addition, a separate manuscript was published demonstrating the use of the measures in a subset of hospitals in the MQii Learning Collaborative implementing quality improvement guided by the MQii Toolkit.
The MQii Toolkit was tested over a three-month implementation period in 2016 through a multi-site Demonstration and Learning Collaborative. The Demonstration took pace at a single hospital that received hands-on training and support for the project, and collected data to assess the impact of using the Toolkit. A paper was published in 2018 outlining the approach and results of the testing efforts. By contrast, a five-hospital Learning Collaborative implemented use of the Toolkit and tracked results with limited support, in order to understand how the Toolkit is adopted and used under real-world circumstances. Findings from this initiative informed revisions to increase the Toolkit’s content, adaptability, usability, and functionality. The revised Toolkit was then tested again by a 50-hospital Learning Collaborative in 2017.
The Toolkit’s use demonstrated that the introduction of recommended malnutrition quality improvement actions helps hospitals achieve performance goals in nutrition care.
Current evidence on malnutrition demonstrates a higher risk, prevalence, and burden of malnutrition among the older adult population (individuals ages 65 years and older). Accordingly, the tools and resources were developed with the 65+ population in mind. Yet, these tools are relevant and applicable for all hospitalized adults (aged 18 years and older) and may also have implications for post-institutional care. In 2020, a paper was published outlining the utility of these measures to understand differences in nutrition care and prevalence of malnutrition across hospital services.
The screening eCQM is specified for all hospitalized adults aged 18+, while the nutrition assessment, care plan development, and diagnosis eCQMs are specified for hospitalized patients aged 65+. However, these three eCQMs can be modified and used to evaluate the quality of malnutrition care among this broader patient population of hospitalized individuals aged 18+ if desired.
Web links to useful tools and resources that may help your implementation efforts can be found throughout the Toolkit. Resources addressing various aspects of malnutrition care — from education about malnutrition’s prevalence and economic impact, to daily quality improvement implementation, to clinical guidelines — can be accessed in the Resource Repository section of the MQii website. Resources include tools for different provider types (e.g., physicians, nurses, dietitians), and address the full spectrum of patient care from admission to discharge. Materials include handouts, presentations, and informational videos.
Some examples of additional resources available include:
Typically, if senior leadership approves the project, then IT participation will be easy to facilitate. You should work with senior leadership to contact the director of IT or Clinical Informatics. Alternatively, if you already have a relationship with IT, you can reach out to them directly. You should inform them of the information you will need, and request an IT team member to serve as your point of contact. Some health systems also have a Performance Improvement (or Quality) Department that may be able to establish a performance data collection and analysis process for the eCQMs. This could serve as an alternate approach if it is difficult to gain assistance from IT to collect the eCQM performance data and assess your quality of care.
This varies based on the skill set and knowledge of the IT personnel and their familiarity with the nutrition templates and components in the EHR. However, in most scenarios the report can be built and tested in about 36-48 hours of staff time that typically stretches across 1-2 weeks overall depending on project prioritization and existing staffing resources. In some situations, you may uncover more testing and refinement is needed, which could take up to an additional week’s worth of time.
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
Members Area
{kind=link}