Malnutrition Care Score for IQR
The Malnutrition Care Score quality measure is available for 2025 hospital reporting.
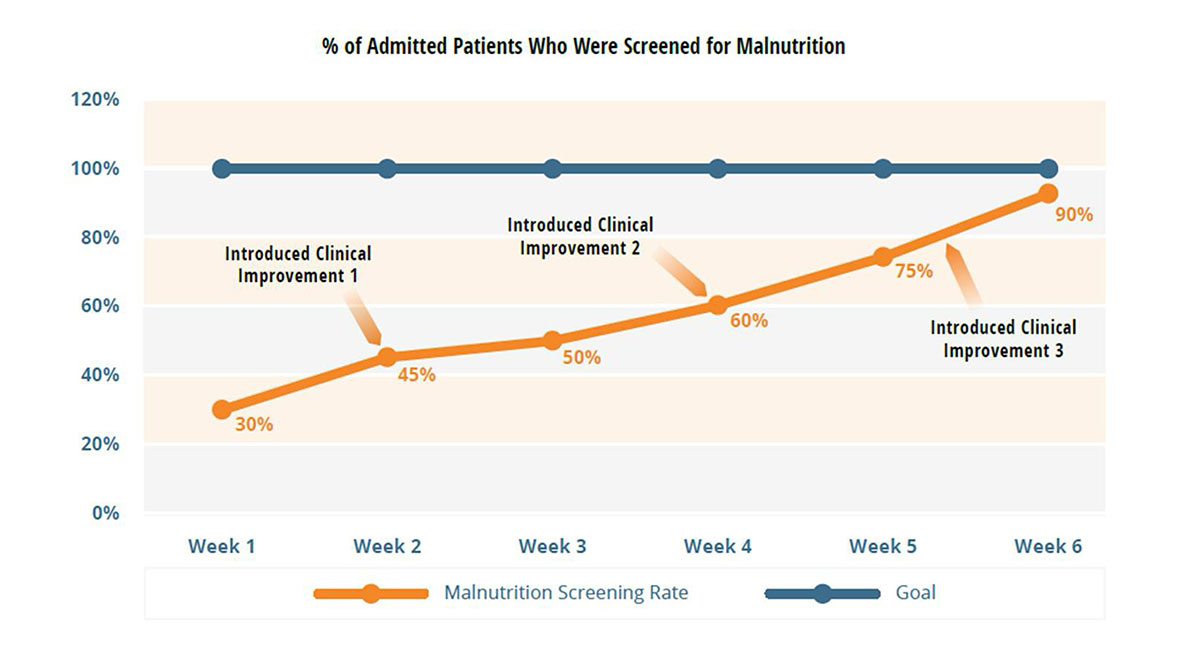
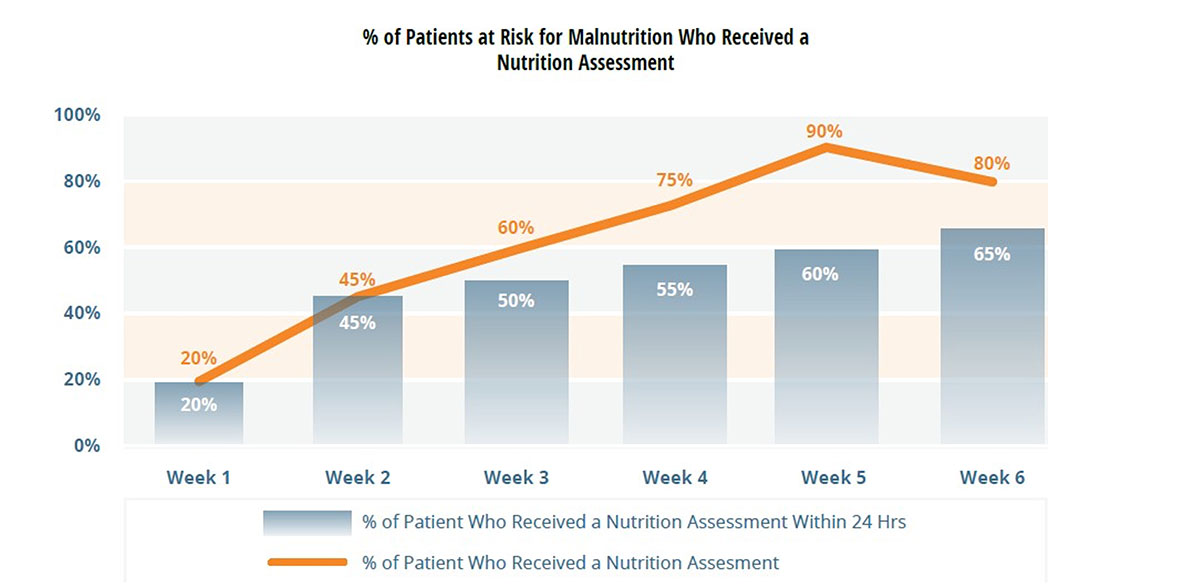
The MQii is designed to help your organization improve
malnutrition care and subsequently achieve better outcomes.
malnutrition care and subsequently achieve better outcomes.